One thing that we’re learning in the Trump era is how extensively government power flows throughout our society, as corporations, universities, and law firms scurry to obey the rules that the new administration is putting forward. A few months ago, I found one of these levers in the form of a fee that doctors must pay when they submit medical bills to Medicare or Medicaid. It’s a classic economic termite, a charge that is relatively small such that consumers don’t notice, but one that fosters a significant amount of money for the monopolist. But in this case, there’s a political twist.
But first, let’s go to the problem itself. In January, a reader sent me a note about a fee paid by her father, a licensed marriage and family therapist. Here’s what she said.
Last year, SimplePractice sent out a note to its customers announcing this fee structure, to widespread anger. One therapist noted on Reddit, “I may get hate for this but this is the kind of shit that really makes me want to surrender my license and become a life coach, allowing me to continue helping people but opting out of the racket. I’m so tired of feeling exploited.” Another said, “Like wtf, being in private practice is already hard and expensive enough, these little ass fees add up. I might drop emr and go back to paper.”
CPT codes are a way to explain what a clinician did during an interaction with a patient. For instance, the most common CPT code for psychologists is 90837, which is the number that means the clinician provided an hour of psychotherapy. To get payment, they will submit this code to health insurers, whether private, Medicare, or Medicaid, and everyone involved will know what it means. First developed in 1966 for use with Medicare, the demand for extensive medical documentation is now a serious contributor to physician burnout, as "[f]or every 8 hours of scheduled patient time, ambulatory physicians spend more than 5 hours on the electronic health records." (...)
In other words, the AMA isn’t offering a software product. It just runs this process, keeping a list of codes that map to different medical procedures. You would think it would be free, a standard for everyone to use. But it’s not, and the AMA is able to charge a royalty for the license to use those codes. Every medical software company seems to have CPT codes and royalties built into their workflow.
Other similar systems are public. For instance, there’s the World Health Organization's International Classification of Diseases (ICD) codes, which are used by most other countries for free. ICD and CPT codes are complements, not substitutes. ICD is a list of diagnoses- “this patient has depression” “this patient has a pulmonary embolus” while CPT is a list of procedures “I talked to this patient for 60 min” “I did this surgery on this patient.” Most billing systems require both codes, basically the insurer is saying “what did you do” (CPT) and “why” (ICD)? But only one is copyrighted. To put it differently, this situation is a bit like if Fedex owned and designed the zip code system, and got to charge anyone who used a zip code.
The total amount of money to the AMA is relatively small, at least compared to overall cost in our health care system. It’s roughly $300 million a year to the AMA in royalty payments. That’s not nothing; but the impact is far more significant on the politics of health care. To understand why, it helps to start with the importance of this particular trade association.
The AMA is the “doctor’s lobby,” and it has been a powerful force in American politics since it was founded in 1847. The rich American doctor was a 20th century community leader, or a petty tyrant, whichever you might believe. Americans respected their physicians, and doctors were conservative and locally rooted, able to speak with authority on matters of public health. They generally feared the state, but also feared corporate control.
The AMA, as such, jealously guarded this position, routinely opposing government attempts to provide universal health care through a centralized administrative public apparatus, haranguing Democrats as seeking to foster “socialized medicine.” And it worked. The AMA beat Franklin Delano Roosevelt, it beat Harry Truman, and it beat Bill Clinton. The threat of corporatization was perceived by medical professionals as coming from the left.
But in the last 20 years, this dynamic has changed, because most doctors now work for large corporations. The old days of hanging up a shingle in a solo or even small group practice is gone because it’s no longer possible for an individual to bargain with the giants that manage the reimbursements, hospital systems, and payment arrangements necessary to be a doctor. Curiously, the AMA, which one would think has some interest in opposing the mass corporatization of its membership, doesn’t seem to care. For instance, the AMA only took a stance on private equity two years ago, long after its membership had transitioned from majority independent practitioners to majority corporate employees. And a key reason might be because it doesn’t make its money by serving doctors anymore. It makes it from the CPT code monopoly it uses to extract from doctors.
Let’s look at some numbers.
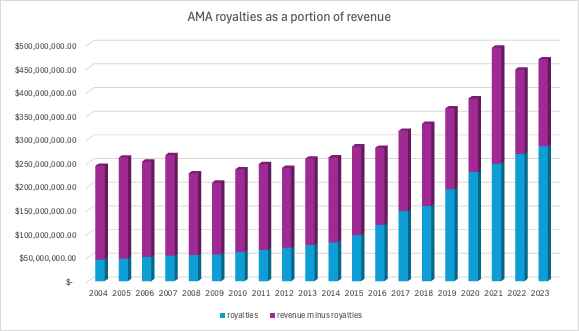
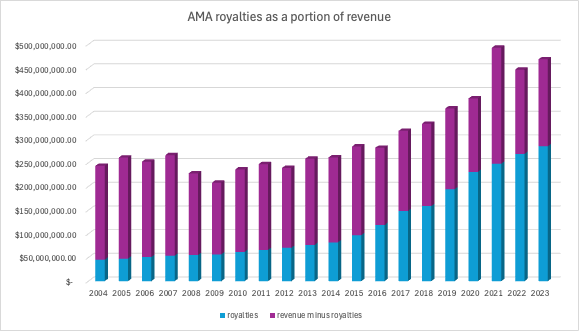
If you look at AMA financial disclosures from 2004 to 2023, you’ll notice three big trends. First of all, dues membership is down. In 2004, it was at $48 million. By 2023, it fell to $33 million. Second of all, revenue is way up, from $243 million to $468 million. And third, there’s an item - “royalties” - that explains it. Royalties, which come largely from CPT code revenue, were about a fifth of the AMA revenue in 2004, at $45 million. In 2023 they were at $308 million, 62% of all revenue, including all the profit, most of the overhead, and the lucrative executive salaries, which have increased by 10x since 2004.
The original CPT codes came out in 1966 to coincide with Medicare, but were published as a book updated annually. It was when electronic medical records took off that the revenue stream picked up. (...)
This situation isn’t just a case of unfair rent extraction, though it is certainly that. It’s also a case of political capture of the AMA. At any point, the Secretary of HHS could choose to revisit its standardization on top of CPT codes, and either foster an alternative, allow competition, or demand that the AMA cut prices. There are alternatives. There are ICD codes. There’s also something called SNOMED, which stands for the Systematized Nomenclature of Medicine – Clinical Terms, which is paid for by at a national level. It’s much cheaper than the CPT codes; Japan, for instance, pays less than $1 million. Switching over to a new system, or even allowing a new system would take a lot of effort. A much simpler change would be Congress passing a law invalidating copyrights for public medial standards, such as CPT codes. It’s ridiculous that a public standard on which everyone must operate is subject to extractive royalty payments. The government has a lot of power here, and could actually start to exert it.
But first, let’s go to the problem itself. In January, a reader sent me a note about a fee paid by her father, a licensed marriage and family therapist. Here’s what she said.
In his practice my dad uses a billing software called SimplePractice and in December they started charging a yearly $20 fee to each clinician. They say this fee is to cover the $18 royalty AMA charges SimplePractice for each clinician who uses the software since the software can use CPT codes, as well as a $2 processing fee.Sure, enough, I went to SimplePractice’s website, and there it is explaining the annual $20 charge for something called a Current Procedural Terminology (CPT) code. SimplePractice says customers must pay the royalty to the American Medical Association, which “owns the rights to CPT codes and mandates the collection of royalty fees for all clinicians who have access to the codes, regardless of usage.”
Last year, SimplePractice sent out a note to its customers announcing this fee structure, to widespread anger. One therapist noted on Reddit, “I may get hate for this but this is the kind of shit that really makes me want to surrender my license and become a life coach, allowing me to continue helping people but opting out of the racket. I’m so tired of feeling exploited.” Another said, “Like wtf, being in private practice is already hard and expensive enough, these little ass fees add up. I might drop emr and go back to paper.”
CPT codes are a way to explain what a clinician did during an interaction with a patient. For instance, the most common CPT code for psychologists is 90837, which is the number that means the clinician provided an hour of psychotherapy. To get payment, they will submit this code to health insurers, whether private, Medicare, or Medicaid, and everyone involved will know what it means. First developed in 1966 for use with Medicare, the demand for extensive medical documentation is now a serious contributor to physician burnout, as "[f]or every 8 hours of scheduled patient time, ambulatory physicians spend more than 5 hours on the electronic health records." (...)
In other words, the AMA isn’t offering a software product. It just runs this process, keeping a list of codes that map to different medical procedures. You would think it would be free, a standard for everyone to use. But it’s not, and the AMA is able to charge a royalty for the license to use those codes. Every medical software company seems to have CPT codes and royalties built into their workflow.
Other similar systems are public. For instance, there’s the World Health Organization's International Classification of Diseases (ICD) codes, which are used by most other countries for free. ICD and CPT codes are complements, not substitutes. ICD is a list of diagnoses- “this patient has depression” “this patient has a pulmonary embolus” while CPT is a list of procedures “I talked to this patient for 60 min” “I did this surgery on this patient.” Most billing systems require both codes, basically the insurer is saying “what did you do” (CPT) and “why” (ICD)? But only one is copyrighted. To put it differently, this situation is a bit like if Fedex owned and designed the zip code system, and got to charge anyone who used a zip code.
The total amount of money to the AMA is relatively small, at least compared to overall cost in our health care system. It’s roughly $300 million a year to the AMA in royalty payments. That’s not nothing; but the impact is far more significant on the politics of health care. To understand why, it helps to start with the importance of this particular trade association.
The AMA is the “doctor’s lobby,” and it has been a powerful force in American politics since it was founded in 1847. The rich American doctor was a 20th century community leader, or a petty tyrant, whichever you might believe. Americans respected their physicians, and doctors were conservative and locally rooted, able to speak with authority on matters of public health. They generally feared the state, but also feared corporate control.
The AMA, as such, jealously guarded this position, routinely opposing government attempts to provide universal health care through a centralized administrative public apparatus, haranguing Democrats as seeking to foster “socialized medicine.” And it worked. The AMA beat Franklin Delano Roosevelt, it beat Harry Truman, and it beat Bill Clinton. The threat of corporatization was perceived by medical professionals as coming from the left.
But in the last 20 years, this dynamic has changed, because most doctors now work for large corporations. The old days of hanging up a shingle in a solo or even small group practice is gone because it’s no longer possible for an individual to bargain with the giants that manage the reimbursements, hospital systems, and payment arrangements necessary to be a doctor. Curiously, the AMA, which one would think has some interest in opposing the mass corporatization of its membership, doesn’t seem to care. For instance, the AMA only took a stance on private equity two years ago, long after its membership had transitioned from majority independent practitioners to majority corporate employees. And a key reason might be because it doesn’t make its money by serving doctors anymore. It makes it from the CPT code monopoly it uses to extract from doctors.
Let’s look at some numbers.
If you look at AMA financial disclosures from 2004 to 2023, you’ll notice three big trends. First of all, dues membership is down. In 2004, it was at $48 million. By 2023, it fell to $33 million. Second of all, revenue is way up, from $243 million to $468 million. And third, there’s an item - “royalties” - that explains it. Royalties, which come largely from CPT code revenue, were about a fifth of the AMA revenue in 2004, at $45 million. In 2023 they were at $308 million, 62% of all revenue, including all the profit, most of the overhead, and the lucrative executive salaries, which have increased by 10x since 2004.
The original CPT codes came out in 1966 to coincide with Medicare, but were published as a book updated annually. It was when electronic medical records took off that the revenue stream picked up. (...)
This situation isn’t just a case of unfair rent extraction, though it is certainly that. It’s also a case of political capture of the AMA. At any point, the Secretary of HHS could choose to revisit its standardization on top of CPT codes, and either foster an alternative, allow competition, or demand that the AMA cut prices. There are alternatives. There are ICD codes. There’s also something called SNOMED, which stands for the Systematized Nomenclature of Medicine – Clinical Terms, which is paid for by at a national level. It’s much cheaper than the CPT codes; Japan, for instance, pays less than $1 million. Switching over to a new system, or even allowing a new system would take a lot of effort. A much simpler change would be Congress passing a law invalidating copyrights for public medial standards, such as CPT codes. It’s ridiculous that a public standard on which everyone must operate is subject to extractive royalty payments. The government has a lot of power here, and could actually start to exert it.